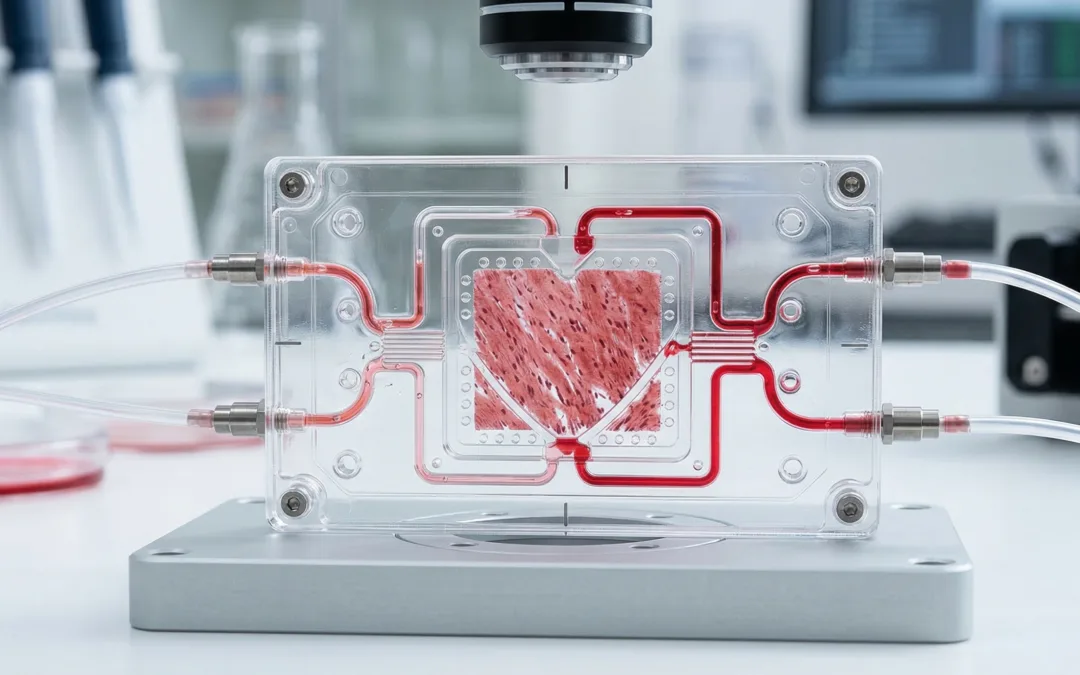
Heart-on-a-chip has become one of those terms mentioned a lot, but it is worth slowing down and asking what it really means. At its core, it is an attempt to build a small in vitro cardiac system that behaves more like tissue and less like a simple cell culture experiment. Instead of putting heart cells on a flat plastic surface and measuring one narrow response, researchers build a structured environment around them. That environment might include soft materials, fluid flow, electrical stimulation, patterned geometry, or some kind of mechanical loading.
That matters because the heart is not a static organ. Its cells are constantly working within a mechanical setting. They shorten, relax, respond to force, and behave differently when the surrounding material or loading conditions change. A simple culture system can still be useful for some questions, but it leaves out much of that physical context.
A lot has changed in this area in a relatively short time. Cardiac cells derived from stem cells are more usable than they were a few years ago. Materials for building these systems are easier to tune. Fabrication methods are also more practical than they used to be. That combination has made it possible to build cardiac models that beat, can be stimulated in controlled ways, and provide better functional data than older in vitro formats.
Why heart-on-a-chip technology matters
Most cardiac research still starts with standard in vitro methods because they are familiar and efficient. That makes sense. The problem is that those systems simplify the environment so much that some important aspects of cardiac behaviour get lost. Cells on rigid plastic are not experiencing the same surroundings they would in real tissue.
Heart-on-a-chip platforms are useful because they bring some of that missing context back into the experiment. They make room for more of the conditions that shape cardiac function, whether that means tissue alignment, soft support materials, fluid movement, pacing, multicellular organization, or some form of mechanical loading and sensing.
Not every system tries to do all of that at once. In many cases, it would not need to. But even bringing back part of that complexity can make the model more informative, especially when the question involves contraction, drug effects, or tissue-level dysfunction.
What a heart-on-a-chip system is trying to recreate
It helps to think of heart-on-a-chip as a model built around a specific part of cardiac function, not as a miniature copy of the whole organ. One setup might be designed mainly to look at beating. Another might be more useful for electrophysiology. Others are built for questions around fibrosis, fluid flow, toxicity, or how engineered tissue handles mechanical stress.
Even though the designs vary, the same basic issues come up again and again.
One is how the cells are arranged. Cardiac cells do not behave the same way when they are dispersed and unstructured as when they are organized more like tissue.
Another is the material around them. Heart cells are sensitive to the stiffness of what they are attached to or embedded in, and that can change how they spread, mature, and function.
The third is movement and load. Cardiac tissue is always working against some kind of physical resistance. A model does not need to copy every detail of the heart to be useful, but if mechanics are left out completely, the picture starts to get thin.
Materials and design choices matter more than they first appear
A heart-on-a-chip platform is only partly about cells. The rest of the story is the structure built around them.
Researchers often use soft polymers, elastomers, or hydrogel-based materials to support engineered cardiac tissues. These materials are chosen for different reasons. Some are easy to fabricate. Some are transparent and useful for imaging. Some offer better compliance or cell compatibility. In many cases, the material is doing more than holding the cells in place. It is shaping how the cells organize, how they beat, and how force is transmitted through the construct.
Geometry matters too. A microchamber, a suspended strip, a patterned surface, or a thin soft membrane all create different physical conditions. Even small changes in size or layout can change what kind of data the model gives back.
That is one reason two papers can both say “heart-on-a-chip” and still be doing very different things.
Heart-on-a-chip in disease modeling
This is probably where heart-on-a-chip becomes most useful. A lot of cardiac disease is not just about what one cell does on its own. It shows up through how cells behave together as tissue, how they handle load, and how they respond over time in a structured environment.
Researchers use these systems to look at problems such as:
-
cardiomyopathy
-
fibrosis
-
hypertrophy
-
ischemic injury
-
arrhythmia-related dysfunction
-
vascular contributions to cardiac disease
In some cases, the cardiac cells come from induced pluripotent stem cells, so the model can be built from a patient-specific source rather than a generic cell line. That is one reason these platforms are appealing for more individualized disease studies, especially when inherited factors or variable drug responses are part of the picture.
They are not a replacement for every other model, and they are not trying to be. What they can do is make certain disease questions easier to study in a controlled way that is still closer to tissue behaviour than a simpler culture system.
Drug screening and cardiotoxicity
Drug testing is one of the most practical reasons people care about heart-on-a-chip. Cardiotoxicity remains a major problem in development, and the earlier it is identified, the better.
A stronger in vitro cardiac model can help researchers see:
-
changes in beating behaviour
-
altered contractility
-
rhythm instability
-
toxicity-related decline in tissue function
-
treatment effects over repeated exposure
-
differences between patient-derived cell sources
That does not mean one chip will solve the full drug development problem. But better cardiac models can make early screening more informative and help reduce false confidence from oversimplified assays.
Where mechanical testing fits in


This is the point that is often underwritten in broader discussions of heart-on-a-chip.
A cardiac model is not just a biological construct. It is also a mechanical system. The tissue beats. The matrix deforms. The scaffold resists load to some degree. The contractile output is shaped by stiffness, geometry, and constraint.
So if you want to know whether a heart-on-a-chip platform is meaningful, you cannot look only at marker expression or visual appearance. You also need to ask mechanical questions.
How stiff is the substrate or scaffold?
How does it deform under load?
Does the construct behave consistently over time?
How does the tissue respond when the environment is softened or stiffened?
Does the model relax, creep, or resist deformation in a way that changes the biology?
That is where mechanical testing becomes important.
Mechanical testing is critical for validating heart-on-a-chip models, because cardiac tissue function depends heavily on stiffness, contractility, and load response. CellScale systems can help quantify these properties in both microscale and larger engineered cardiac constructs.
Testing methods that are relevant to heart-on-a-chip systems
Not every testing method applies to every cardiac model, but several are particularly relevant.
Micro-Mechanical Testing
Many heart-on-a-chip constructs are small, delicate, and hydrated. Micro-mechanical testing makes sense when the sample is too small or too soft for more conventional workflows.
Compression Testing
Compression testing can be useful for soft scaffold materials, hydrogel supports, and small engineered tissues where deformation resistance matters.
Biaxial Testing
Some cardiac tissues and sheet-like engineered constructs are loaded in more than one direction. Biaxial testing can be useful when a single-axis view is not enough.
Viscoelastic & Time-Dependent Testing
Engineered cardiac materials often show time-dependent behaviour. Stress relaxation and creep can matter, especially in soft matrices or long-duration studies.
Hydrated and temperature-controlled testing
If the material or construct is meant to behave like living tissue, then dry-room measurements at the wrong temperature may miss the point. Hydrated, physiologically relevant conditions often matter.
Why the mechanical side cannot be treated as optional
People sometimes talk about heart-on-a-chip as if the engineering challenge ends once the cells are alive and beating. But beating alone is not enough. A weak or unrealistic mechanical environment can still distort what the model tells you.
A construct may look organized under a microscope and still be sitting in a matrix that is too stiff. A tissue may respond to a drug in culture and still behave differently once load is introduced. A scaffold may work well on day one and change mechanically over time in ways that alter the biology.
That is why it helps to think of heart-on-a-chip development as part cardiac biology, part materials science, and part biomechanics.
That is also where the connection becomes more concrete. Systems like the BioTester, UniVert, and MicroTester fit into this space because they help researchers characterize soft, hydrated, mechanically active biomaterials and tissue-like constructs in a more quantitative way.
Stem cells and patient-specific models
Stem cell advances have pushed this field forward more than almost anything else. Induced pluripotent stem cell-derived cardiomyocytes allow researchers to build human cardiac models without relying entirely on primary tissue.
That opens up a lot of possibilities:
-
patient-specific disease models
-
inherited cardiac disorder research
-
individualized drug response studies
-
human-cell-based screening workflows
There is still a maturity problem, of course. Many stem-cell-derived cardiomyocytes behave more like immature cardiac cells than adult myocardium. But even with that limitation, these models are often more useful than older systems, especially when the surrounding environment is designed carefully.
What is still difficult
Heart-on-a-chip sounds exciting because it is exciting, but the limitations are real.
Some platforms are hard to standardize.
Some are too custom to scale well.
Some reproduce beating but not realistic force.
Some have good biology but weak mechanics.
Some have great sensing but do not mimic tissue structure very well.
Regulatory adoption is another long-term challenge. For these systems to become more central in screening and development pipelines, they need to be reproducible, comparable, and clearly predictive.
That is a high bar.
Still, the trajectory is strong. Better materials, better cell sources, better fabrication, and better mechanical validation should all help.
Conclusion
Heart-on-a-chip is not just a smaller version of cardiac research. It is a different kind of model, one built to bring together cells, materials, geometry, flow, and mechanics in a more controlled way. Done well, it gives researchers a better window into how cardiac tissue actually behaves, not just how individual cells survive in culture.
That is why the field matters for disease modeling and drug testing, but also why it has to be validated carefully. If the mechanics are wrong, the biology can be misleading. If the environment is too simplified, the readouts lose value.
The strongest heart-on-a-chip systems are the ones that take both sides seriously: the biological side and the physical side.
Related reading: For another example of how mechanically informed tissue models are built with advanced fabrication methods, read our post on the 3D Bioprinted Pterygium Eye Model for Disease Research and Drug Testing.