Overview
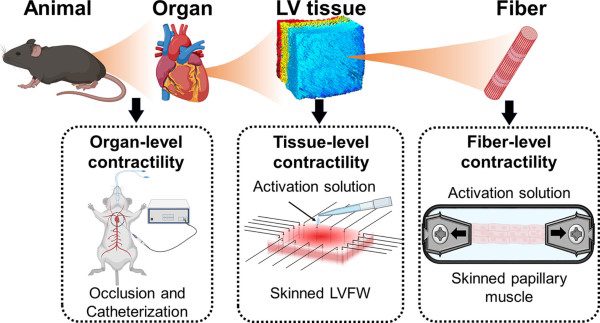
Left ventricle biomechanics cannot be understood at only one scale. Cardiac contraction begins at the sarcomere and myofiber level, but what matters physiologically is how those forces transfer through myocardial tissue architecture and finally appear as organ-level pumping function. That is what makes this Acta Biomaterialia study so useful. Rather than treating the left ventricle as a single mechanical unit, the authors examined myocardial behaviour across fiber, tissue, and organ scales to understand how contractility is translated through the heart wall.
A central part of that workflow was biaxial mechanical testing of murine left ventricle free wall tissue. The study combined passive biaxial stretching, stress relaxation testing, active contraction measurements, papillary muscle fiber testing, and organ-level pressure-volume analysis. Together, those methods created a multiscale view of left ventricle biomechanics that is especially relevant for structural heart disease, systolic dysfunction, and cardiac tissue engineering.
Why left ventricle biomechanics need a multiscale view
The heart does not fail or adapt at just one length scale. Myofiber alignment, extracellular matrix content, passive tissue stiffness, and chamber geometry all influence how local force generation becomes global function. The paper makes this point clearly: understanding myocardial contractility in health and disease requires following force transmission from fiber to tissue to organ rather than relying on one measurement alone.
This is particularly important in structural heart disease. The authors frame their work around conditions such as myocardial infarction and systolic heart failure, where altered contractile patterns can change cardiac function long before a single bulk metric explains why. Their multiscale approach is meant to improve mechanistic understanding and provide better performance metrics for left ventricle function.
How biaxial mechanical testing was used

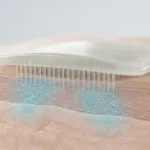
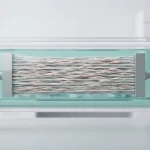
For the tissue-level work, left ventricle free wall specimens were mounted on a CellScale BioTester and tested along the circumferential and longitudinal directions. The workflow included passive biaxial tensile tests, biaxial stress relaxation tests, and then active testing after chemical skinning. The passive tests included equibiaxial loading and non-equibiaxial stretch ratios, with specimens submerged in relaxation buffer to prevent dehydration.
Planar biaxial mechanical testing is especially valuable here because left ventricle tissue is anisotropic. It does not behave the same in all directions, and uniaxial methods would miss important direction-dependent responses. In this study, biaxial testing allowed the researchers to compare circumferential and longitudinal behaviour directly under passive and active conditions, which is exactly the kind of data needed to study anisotropic tissue mechanics in the myocardium.
Key findings in left ventricle tissue mechanics
1. Passive and active myocardial behaviour are not the same story
One of the most useful results is the contrast between passive and active behaviour. Passive testing showed fairly similar behaviour in the circumferential and longitudinal directions, with only a modest circumferential bias. Active testing, however, showed significantly larger active stresses in the longitudinal direction. That means the directional mechanics of the left ventricle look different depending on whether the tissue is simply being stretched or actively contracting.
2. Tissue-level stress was much lower than fiber-level stress
Papillary muscle fibers generated maximum stresses on the order of 42.3 ± 1.46 kPa, while the left ventricle free wall tissue developed substantially lower active stresses. The paper explains this difference through tissue composition and architecture: non-contractile constituents, extracellular matrix, fiber rotation through the wall thickness, and force transmission across a branching myocardial network all reduce how much fiber-level force appears as tissue-level stress.
3. Passive stretch influenced active force development
The study also showed that active stress development depended on the initial passive stretch of the tissue. When specimens were pre-stretched, total stress during active contraction increased, consistent with length-dependent myocardial behaviour and the broader logic behind the Frank-Starling mechanism. In other words, passive state and active state are mechanically linked, which matters when interpreting diseased myocardium with altered relaxation or stiffness.
4. Active relaxation behaved differently from passive relaxation
Passive viscoelastic relaxation was relatively similar between the two tissue directions. Active relaxation was not. The myocardium relaxed faster in the direction with the larger peak active stress, highlighting that active vs passive myocardial behaviour should not be treated as interchangeable mechanical phenomena. That distinction is important for disease models involving impaired relaxation.
What the multiscale comparison adds
A major strength of this work is that it does not stop at ex vivo tissue mechanics. The authors also compared fiber-level and tissue-level findings with organ-level contractility from pressure-volume measurements. Their conclusion is not that all three scales look identical, but that tissue-level measurements can still be meaningfully connected to organ-level function. That supports the value of ex vivo myocardial testing for studying cardiac function, disease mechanisms, and translational model development.
This is where the paper becomes more than a mechanics study. It becomes a framework for asking how local myocardial changes contribute to global dysfunction. For researchers working on infarction, heart failure, engineered cardiac tissues, or computational heart models, that is a very practical contribution.
Why this matters for cardiac biomechanics research
Studies of left ventricle biomechanics often emphasize chamber-level outputs such as pressure, strain, or ejection performance. Those are valuable, but they do not fully explain how the myocardium is behaving as a material. This paper shows why tissue-level assays still matter. They capture anisotropic tissue mechanics, reveal differences between passive and active myocardial behaviour, and help explain how architecture and extracellular content shape contractility.
It also highlights the role of biaxial testing in cardiac biomechanics. When the question is how myocardial tissue carries load in more than one direction, biaxial mechanical testing is not just a nice option. It is often the method that best matches the biology.
How the BioTester fit this study
The BioTester enabled controlled biaxial loading of left ventricle free wall tissue along physiologically relevant directions, allowing the researchers to characterize passive tensile behaviour, stress relaxation, and active contraction in the same overall workflow. In this study, that made the instrument part of a broader multiscale pipeline rather than just a standalone test platform.
For cardiac tissue mechanics research, that is the real takeaway. The value is not simply that the tissue can be stretched in two axes. It is that biaxial testing helps bridge structure, mechanics, and function in a way that is directly relevant to how the heart actually works.
Related reading
If you want to learn more about how biaxial methods are used in cardiac research:
-
For another example of how biaxial loading is used to study heart tissues, see our post on biaxial heart tissue testing at the University of Denver.
-
For a broader overview of test selection and method fit, explore our guide to mechanical testing of biomaterials.
-
If your focus is valve mechanics rather than ventricular wall behaviour, you may also like our article on mechanical properties of heart valve leaflets.